
What are Electronic Health Records?
- Home
- Insights
- Article
- What are Electronic Health Records?
Qualitative Research Service
News & Trends
Recommended Reads

Data Collection
As the data collection methods have extreme influence over the validity of the research outcomes, it is considered as the crucial aspect of the studies
- 1. Introduction
- 2. DeepHealth’s Diagnostic Suite™: Revolutionizing Radiology Workflows
- 3. Key Features
- 4. AI Impact on National Screening Programs
- 5. SmartMammo™: Enhancing Breast Cancer Screening
- 6. DeepHealth AI Use Cases Across Specialties
- 7. Strategic Collaborations and Ecosystem Expansion
- 8. Impact and Adoption of DeepHealth’s AI Solutions
- 9. Conclusion: The Future of Radiology with AI
- 10. References
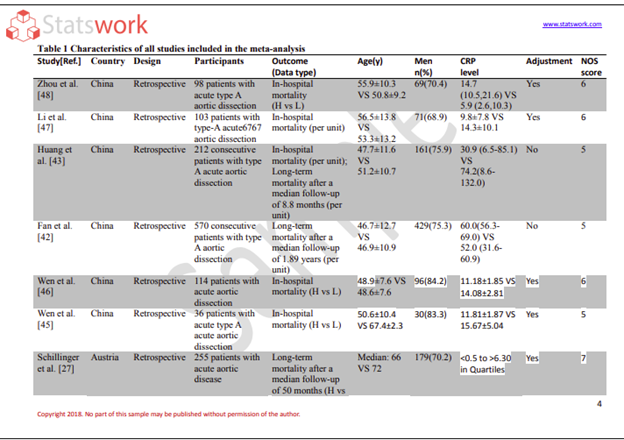
Healthcare practitioners maintain electronic longitudinal records (referred to as “EHR” or an Electronic Health Record system) of their clients’ health information over the client’s lifetime. These records aim to improve the quality, efficiency, and accessibility of health care and promote continuity in the delivery of care.[1]
Essential Features of Electronic Health Records
The EHR contains a comprehensive database of standardized patient information, which includes:
- Demographic information (age, sex, and telephone number).
- Patient medical history, diagnosis, and problem lists.
- Prescribed medications and allergy documentation.
- Lab test and imaging results.
- Clinical notes, treatment plans, and discharge summaries.
- Immunization history and preventive care documentation.
These elements create a complete picture of a patient’s overall health condition.[2]
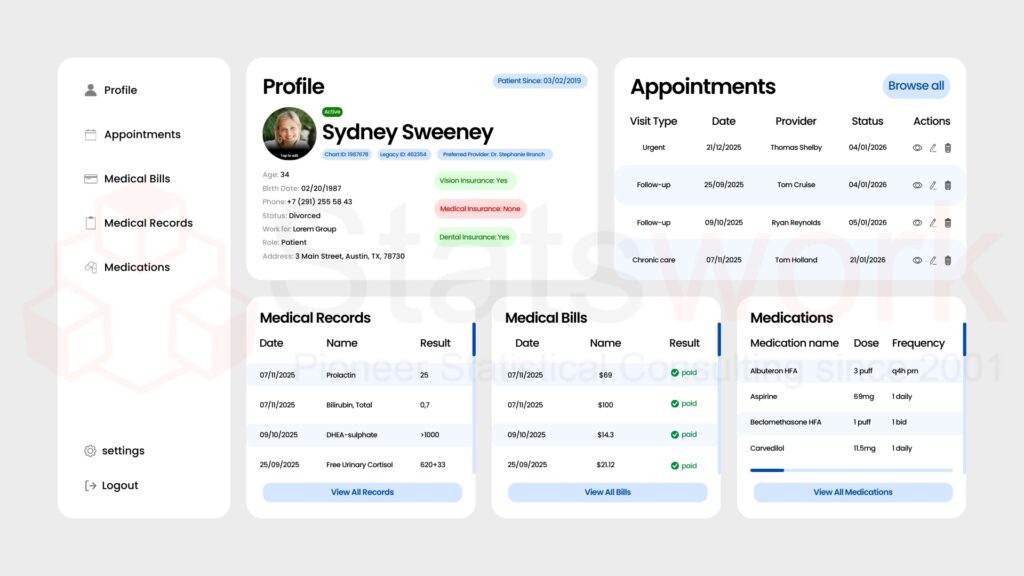
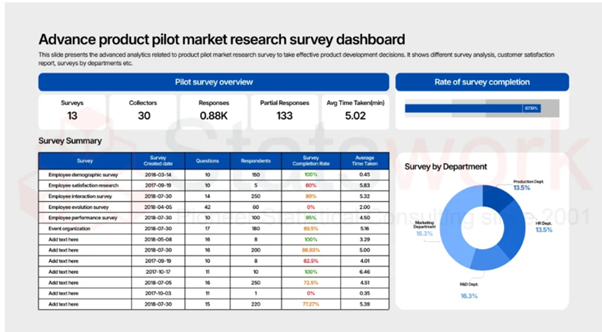
Fig. 1 shows a patient Electronic Health Record dashboard with medical records, bills, medications, and appointments.
Positive Outcomes of Electronic Health Records in Healthcare
Electronic Health Records Offer Benefit to Healthcare Providers and Patients in Many Ways:
- Improved Clinical Decision-Making: Helps healthcare providers get real-time, accurate patient data, allowing them to make timely decisions on patient treatment.
- Reduced Medical Errors: Eliminates the risk of errors caused by poor handwriting, incomplete records and duplicate data.
- Enhanced Care Coordination: Provides a method for exchanging patient information easily between providers, labs and hospitals.
- Operational Efficiency & Better Outcomes: Provides an efficient way to manage the flow of paperwork and provides a foundation for managing population health and doing research to improve patient care.[2]
Paper Records vs Electronic Health Records
Aspect | Paper Records | Electronic Health Records |
Accessibility | A place-based only option. | Remote access for authorized personnel only. |
Data Sharing | Time-consuming manual entry. | Secure and instant exchange of data. |
Storage | Requires physical space for filing storage. | Data stored digitally along with backup. |
Error Risk | Handwriting issues lead to high potential for errors. | Reduction of potential for errors through standard entry process. |
Data Security | Potentially lost or damaged. | Securely protected with encryption and access control.[3] |
Interoperability and Data Sharing
A defining characteristic of Electronic Health Records (EHR) is interoperability
- Provides a seamless exchange of data among different healthcare organizations
- Enables continuity of patient care across multiple providers (e.g., if a patient has changed providers, their medical information can easily transition to their new provider).
- Enables integration with laboratories, pharmacies, imaging centers, etc.
- Enables quicker diagnosis and treatment decisions for patients.
Interoperability allows patients to keep track of the medical information as they travel through their care journey.[4]
Role of EHRs in Regulatory Compliance and Analytics
Electronic Health Record Systems Provide Support for Healthcare Organizations in the Following Ways
- Ensuring that Healthcare Organizations Comply with the Appropriate Regulatory Compliance, Standards, and Guidelines.
- Providing Healthcare Organizations with Audit-Ready Clinical Documentation.
- Enabling Healthcare Organizations to Use Data Analytics to Improve Quality of Care Through Continuous Improvement Activities.
- Supporting Clinical Research and Population Health Initiatives.
Healthcare Providers can Utilize Electronic Health Record Data to Improve Patient Outcomes while Still Complying with Regulatory Compliance Standards.[5]
Therefore, EHRs improve the quality of care through increased accuracy, coordination of care, collaboration between providers, quality, and compliance which results in increased safety, efficiency, and patient-centered care when making clinical decisions in today’s healthcare organizations.
Power your research with StatsWork Biostatistics—precise analytics, faster insights, and data-driven confidence from protocol to approval.
Reference
- Hoerbst, A., & Ammenwerth, E. (2010). Electronic health records. Methods of information in medicine, 49(04), 320-336. https://www.thieme-connect.com/products/ejournals/abstract/10.3414/ME10-01-0038
- Keyhani, S., Hebert, P. L., Ross, J. S., Federman, A., Zhu, C. W., & Siu, A. L. (2008). Electronic health record components and the quality of care. Medical care, 46(12), 1267-1272. https://journals.lww.com/lww-medicalcare/abstract/2008/12000/electronic_health_record_components_and_the.11.aspx
- Tsai, J., & Bond, G. (2008). A comparison of electronic records to paper records in mental health centers. International Journal for Quality in Health Care, 20(2), 136-143. https://academic.oup.com/intqhc/article-abstract/20/2/136/1785685
- Bhartiya, S., Mehrotra, D., & Girdhar, A. (2016). Issues in achieving complete interoperability while sharing electronic health records. Procedia Computer Science, 78, 192-198. https://www.sciencedirect.com/science/article/pii/S1877050916000351
- Chianumba, E. C., Ikhalea, N., Mustapha, A. Y., Forkuo, A. Y., & Osamika, D. (2024). Enhancing corporate governance and pharmaceutical services through data analytics and regulatory compliance. International Journal of Advanced Multidisciplinary Research and Studies, 4(6), 1613-1619. https://www.multiresearchjournal.com/admin/uploads/archives/archive-1744636672.pdf