
Quantitative report writing
Results and Discussion
Obesity, its attendant health consequences and the consequent health burden, are expected to reach epidemic proportions in developing countries such as India, particularly in some sections of the population. Overweight and obesity in children and adolescents can no longer be considered as factors reflecting the economic development and the attainment of food adequacy in developing societies. Childhood obesity is the prelude to a public health disaster that we will have to deal with in this 21st century. The present thesis was done in an effort to test the hypothesis – Is there any significant influence of diet or its constituents in contribute to overweight or obesity in the adolescents. And if so are there any differences in the dietary pattern among adolescents coming from different household income levels. The results are summarized using the described statistical means and are described below.
Nutritional profile of adolescents based on household income
The subjects chosen were 200 consisting of 100 boys and 100 girls. To have wider variety in the standards of living, adolescents from a government school and a private school were selected as explained in the methodology. The basic data on their anthropometric parameters and nutrient profile are outlined in the Table -1. Adolescents were categorized into boys and girls and were further grouped based on their household income levels as <2000 Rs/month; 2000-5000 Rs/month and >5000 Rs. The mean age of the boys in these 3 household categories were 14.6 yrs, 15.8yrs and 14.9 yrs respectively. Similarly the mean age of the girls was 13.7yrs, 15.4 yrs and 16 yrs. BMI increased as the household income increased both in the case of boys and girls (Boys <2000Rs=20 kg/m2; 2000-5000 = 21kg/m2; >5000 =21 kg/m2; Girls <2000rs=17.8 kg/m2; 2000-5000 = 19.9kg/m2; >5000 =20.6 kg/m2). There was an increase in SFA% and mean fat % of total calories both among boys and girls across all income levels (Boys <2000rs=8.1 & 28.3; 2000-5000 = 8.3 & 25.5; >5000 =9.4 & 27.4; Girls <2000rs=7.8 & 25.6; 2000-5000 = 9.2 & 28.4; >5000 =9.7 & 27.8) as shown in figure 3&4. Similarly the waist and hip circumference of both boys and girls are also increasing as shown in Fig 1 &2.
Table I:Basic Anthropometric and Nutrient profile of the adolescents based on Household income (n=200)
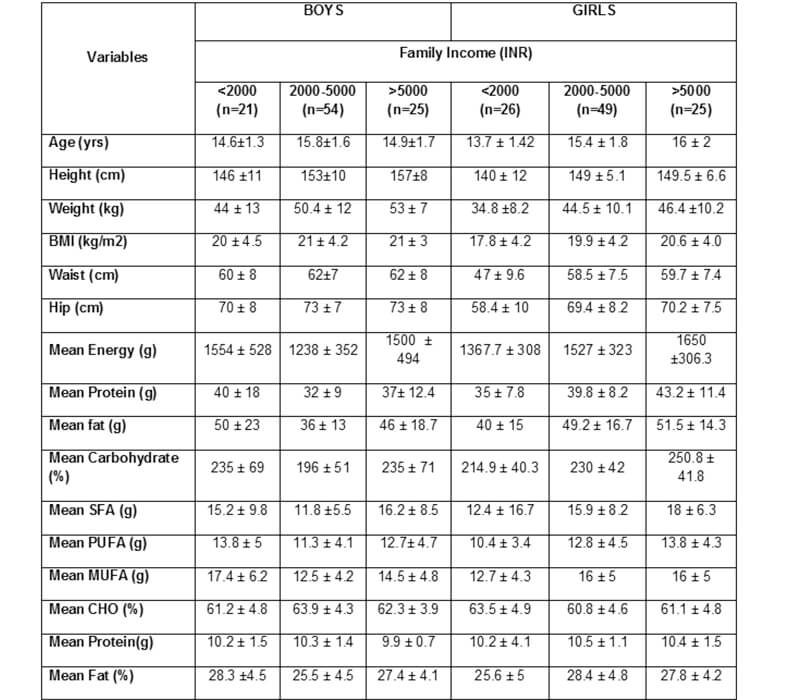
figure 1

figure 1

figure 1

figure 1

Nutritional profile of adolescents based on their BMI cut off values (healthy weight <85th percentile and over weight > 85th percentile)
Of the chosen 200 subjects 179 subjects were healthy BMI ie., below the 85th percentile and 21 subjects were overweight (>85th percentile). Waist circumference was significantly higher among the overweight category as compared to the healthy weight subjects (p<0.001) as shown in Table 2 and Fig VI.
Table II : Anthropometric and nutrient profile of the adolescents based on the BMI cut off (below and above 85th percentile)

Data are mean ± SD , * p< 0.05, ** p< 0.001 statistically significant
Figure VI

Similarly the WHR also showed significant difference between healthy and overweight subjects (Table 2). It was of interesting to note that the mean visible fat intake was almost double in the overweight category (<85th percentile 7g vs >85th percentile 13g). Data also shows higher percentage of calories as SFA and total fat (<85th percentile Total fat 27% >85th percentile 30%; <85th percentile SFA 9% and >85th percentile 10%) taken by the overweight subjects (Table 2; Fig V).
Figure V

However there was decreased intake of carbohydrates as %calories by the overweight subjects (<85th percentile CHO% 63% vs 60% in >85th percentile).
Dietary pattern
The chosen subjects (n=200) were categorized into quartiles of dietary fat intake and the data are shown in the Table 3. The data (Table 3 & Fig VII) showed increase in BMI between 1st and 4th quartile of dietary fat intake (1st quartile of dietary fat BMI = 20.1kg/m2 and the 4th quartile 21.5kg/m2).
Figure VII

Similarly the WHR also showed an increase between 1st and 4th quartile of dietary fat intake (Table 3). Similarly the SFA% and MUFA% were also increased across from the 1st quartile to 4th quartile dietary fat (Table 3 & VIII).
TABLE 3
Baseline characteristics of the adolescents based on dietary fat intake (g) in quartiles

figure VIII

Family History of Diabetes
Adolescent subjects were grouped based on their family history of diabetes. Thus a positive group based on their positive family history and a negative group for the reported absence of diabetes in their family. The data are given in the table 4. The study findings showed that adolescents with the reported positive family history had higher mean waist and hip circumferences than the adolescents with the negative family history of diabetes (Table 4 & Fig IX). WHR showed significant difference between positive and negative categories of adolescents with regards to self reported family history of diabetes.
Figure IX

Again the mean Total Fat% and SFA% were significantly (Total fat p= 0.058) higher among adolescents with positive family history of diabetes (Positive family history of diabetes category mean total fat intake 27.6%; the negative family history of diabetes 26.3%). However the intake of PUFA% was higher among the negative family history reported adolescents (Table 4 and Fig X)
TABLE 4
SELF REPORTED FAMILY MEDICAL HISTORY OF THE CHOSEN ADOLESCENTS (n=200)

Data are mean ± SD , * p< 0.05, ** p< 0.001 statistically significant
Figure X

Adolescents reported with positive family history of diabetes (n=110) were further sub-grouped based on the BMI cut off percentile as <85th and >85th centiles. Based on these subgroup categories their nutrient and anthropometric data was summarized and given in the Table 5. Waist, hip circumferences and WHR were increased significantly (p=0.002, 0.004, 0.054 respectively) among the adolescents from the positive family history of diabetes and whose BMI was greater than 85th percentile. The fat% intake and SFA% intake of total calories were also higher in this group (>85th percentile) than the adolescents from the same positive family history of diabetes, but whose BMI was <85th percentile.
Table 5
Anthropometric and Nutrient profile of the adolescents with positive family medical History based on the BMI cut off (below and above 85th percentile)

Data are mean ± SD , * p< 0.05, ** p< 0.001 statistically significant
The reported positive family history of diabetes among the adolescents studies (n=200) was 43.5%, family history of hypertension was also 43.5%, whereas the reported history of heart problem was 27% and stroke 11.5% (Table 6)
Table 6
Family Medical history of the study subjects (n=200)


Discussion
The present study conducted among randomly selected 200 adolescents (13-18yrs) from the Chennai urban revealed that the overweight in adolescence is catching up and it seems to be related to the household income. Dietary factors such as higher intake of SFA and total fat are also associated with the overweight pattern among adolescent boys and girls. It was also noted in this study that overweight adolescents with positive family history of diabetes had higher intake of SFA% and total fat than normal weight adolescents with the same positive family history of diabetes. Similarly this category of overweight adolescents also had higher waist, hip circumferences and WHR.
Why should we be concerned about overweight in young children and adolescents? Overweight children are more likely to be overweight as adults than are non-overweight children: an overweight 1-or 2 year old child is 1.2 times more likely to be an overweight adult; an overweight 15-17 year old child is 17.5 times more likely (Hitaker, et al.,1997). One review of literature suggested that 26-41% of overweight preschool children become overweight adults (Serdula, et al.,1993). There are many reasons that overweight is one of the most troubling public health problems facing the world today. (Dietz, et al., 1998)
Overweight is associated with a myriad of health problems: high blood pressure, cardiovascular disease, diabetes, respiratory difficulties, joint and sleep problems (Dietz, et al., 1998), psychological and social problems. These problems negatively affect the quality of life of the individual and his/her family and place a burden on our public health system. Overweight children are more likely to have multiple nutrition risks than are non-overweight children: 79.1% of overweight children have two or three nutrition risks, while only 48.2% of non-overweight children have the same number of risks.
Studies by Anand, Tandon and Varma et al from northern India, noted that children with obesity had a high risk of hypertension. In low-income Mexican Americans, the prevalence of overweight in adolescence was 40.1% (Lacar, et al., 2000). A rising trend in the prevalence of obesity in childhood and adolescence has been noted in several studies (Chinn, et al., 2001;.Kromeyer-Hauschild, et al,1999). In Germany, obesity in children has almost doubled between 1975 and 1995 (Kromeyer-Hauschild, et al., 1999). Childhood obesity has important health consequences for children and is a major antecedent of adult obesity (NIH 1995). Several studies have demonstrated the persistence of childhood obesity into adulthood (Serdula, et al., 1993; Siervogel, et al., 1991). The likelihood of adult obesity is greater for obese adolescents (Guo, et al., 1994). Obesity is also associated with abnormal lipid profiles during childhood and adolescence. Other early stages of chronic diseases also relate to obesity, as do increased morbidity and mortality (must et al 1992). Among U.S adolescents aged 12-17years, the level of obesity was relatively constant throughout the 1960s and 1970s but has shifted upward then. (Troiano, et al., 1995) showed that, between the years 1976-1980 and the years 1988-1991, the proportion of adolescents above the 95th percentile more than doubled.
More recent results showed that there was a significant increase in the obesity pattern for adolescents between the first phase of NHANES III (1988-1991) and the second phase (1991-1994) (Popkin,1994; Richard Udry, 1998). Prevalence of overweight was associated with lower physical activity score and higher economic status (Ramachandran, et al.,2002). The present study though did not find the prevalence but did find the mean BMI increasing with increasing household income. The study also found that as affluence increases the dietary fat intake also increased especially saturated fatty acid (SFA- Fig III)
(Moussa, et al., 1999; Musaiger,etal.,1993). had noted that a family history of obesity and diabetes were risk factors for obesity in children. Though the present study did not aim at this, it however observed that adolescents with <85th percentile and with positive family history of diabetes had higher BMI, WHR and also consumed higher total dietary fat and especially saturated fats (SFA) (Table 5)
The present study has highlighted that obesity an emerging problem in adolescent children is likely to be associated with the possible dietary fat intake especially the saturated fats. Overweight and obesity are, however difficult to correct after becoming established, and there is an established risk of overweight during childhood persisting into adolescence and adulthood (FAO,1996). It is increasingly recognized that unhealthy lifestyles do not just appear in adulthood but drive the early development of obesity, dyslipidemia, high blood pressure, impaired glucose tolerance and associated risk. Increased availability of fast foods and faulty eating habits especially fatty food choices have taken place over 30 years. At the same time, the amount of physical activity has been greatly reduced both at home and in school, as well as by increasing use of mechanized transport.
However, the present study had many limitations owing to the time constraint for a detailed study. Hence the present study recommends that further studies are needed to cover wider adolescent population and also to find out the prevalence of overweight and obesity across the various socio economic levels.
Summary and conclusion
About 25% of children are overweight or obese, according to newly established national criteria. These teens are at significant risk for becoming obese adults, and adolescent. Obesity predisposes to a range of medical problems like cardiovascular disease and diabetes. The reason for these alarming changes is due to increasing westernization, urbanization, and mechanization occurring in most developed and also in developing countries around the world is associated with changes in the diet towards one of high-fat, high-energy foods and a sedentary lifestyle (physical inactivity)
Hence, the study was undertaken with the main objective as to assess the Nutritional profile of the adolescents and – it’s implication on health risk. This study was conducted in the city Corporation managed and the other is the private school. To have wider variety in the standards of living, adolescents from a government school and a private school were selected, the subjects were selected based on the convenience of the interviewer and the sample size being 200. The study subjects were divided into two groups as 13-15yrs (50 boys and 50 girls) who were in the high school and 16-18 yrs (50 boys and 50 girls) who were in the higher school level and under graduate level, the subjects were randomized equally from both private and government school. The study was conducted with the help of 24hrrecall and open ended questionnaire to obtain require data. The collected data were analyzed systematically and concluded as follows:
Studies suggest that individuals who were in the 2000-5000Rs and >5000 RS income group had higher level of BMI, WHR, dietary fat and saturated fats. The total fat intake and saturated fatty acid were increased both boys and girls across all the income level but no significant increase or decrease in the protein intake across the income group of both boys and girls were found.
Studies show that higher the intake of saturated fatty acid higher the risk of cardiovascular diseases. In the present study, overweigh subjects had a high fat intake and SFA% from total calories than person with the normal weight. Visible fat intake was almost double in overweight subjects. Overweight subjects showed a higher waist circumference than the normal weight subjects and this difference was statistically significant.
Studies shown that fat intake is directly associated with coronary artery diseases (CHD). In the present study Waist circumference and BMI was high increase with 1st and 4th quartiles of fat. Saturated fatty acid also increases with the increase in quartiles of fat intake.
Studies have shown that risk of obesity is two to three times greater for an individual with a family history of obesity and increases further with severe obesity. In the present study 55% and 45% of the subject’s family was positive and negative family history respectively. Subjects with the family history positive had higher waist and hip than with negative family history. Mean fat and SFA% was higher in positive family history than the other. Polyunsaturated fatty acid was significantly lower in the negative family history.
Studies shown that the risk increases with the subjects of positive family history. In the present study overweight subjects with the positive family history had higher waist and hip circumference than normal weight. Mean fat intake (g), percentage of saturated fatty acids and monounsaturated fatty acids from total calories was higher in the overweight subjects than with normal weight.
Thus it is noted that increasing urbanization, changing lifestyle, increased intake of saturated fat and genetic predisposition might be the reason behind the increase in overweight and obesity in adolescents. Thus Education about the long-term health consequences and risks associated with overweight and how to achieve and maintain a preferred weight is necessary. While many individuals attempt to lose weight, studies show that within five years a majority of them regain the weight. In order to maintain weight loss, good dietary habits must be coupled with increased physical activity, and these must become permanent lifestyle changes.